How Dry Eye Disease Affects OCT Image Quality Through Tear Film Instability
Optical coherence tomography (OCT) has become one of the most valuable tools in modern eye care, allowing clinicians to evaluate retinal structures with remarkable precision. But even the most advanced imaging system depends on one often-overlooked factor: a stable ocular surface. Increasing evidence now shows that dry eye disease (DED) can significantly reduce OCT image quality through tear film instability, creating challenges that may affect both diagnosis and long-term disease monitoring.
For clinicians who rely on OCT to detect subtle retinal or glaucoma progression, understanding the impact of dry eye is becoming increasingly important.
Why Tear Film Stability Matters in OCT Imaging
OCT works by using low-coherence interferometry to generate detailed cross-sectional retinal images. Before light reaches the retina, however, it must first pass through the tear film, cornea, and lens. When the tear film is smooth and stable, light transmission remains clear and consistent. In patients with dry eye disease, that optical pathway becomes irregular.
Tear Film Breakup Creates Optical Distortion
A healthy tear film acts as a smooth refractive surface. In DED, reduced tear film breakup time (TBUT) leads to areas where the tear layer thins or breaks apart entirely. These unstable regions scatter incoming light and introduce optical aberrations during image acquisition.
As a result, OCT scans may show:
- Reduced signal strength and image intensity.
- Increased background noise and motion artifacts.
- Poor retinal layer definition.
- Lower scan reproducibility between visits.
- Artifacts that may mimic retinal pathology.
In many cases, the issue is not the OCT device itself but the unstable tear film disrupting the quality of the captured signal.
The Problem With Dynamic Tear Film Changes
One of the more difficult aspects of dry eye-related imaging issues is that tear film instability changes rapidly. Unlike a fixed opacity such as a cataract or corneal scar, the tear film can fluctuate from second to second during the scan.
A patient may begin the acquisition with acceptable image quality, only for tear breakup to occur midway through the scan. This often leads to inconsistent results, especially in patients who struggle to maintain steady fixation or avoid blinking during imaging.
For technicians and clinicians, this explains why some scans appear excellent one moment and unusable the next.
What the Research Shows
Several recent studies have quantified the effect of dry eye disease on OCT performance. Compared with healthy eyes, patients with moderate to severe DED consistently demonstrate lower imaging quality across multiple parameters.
Reported findings include:
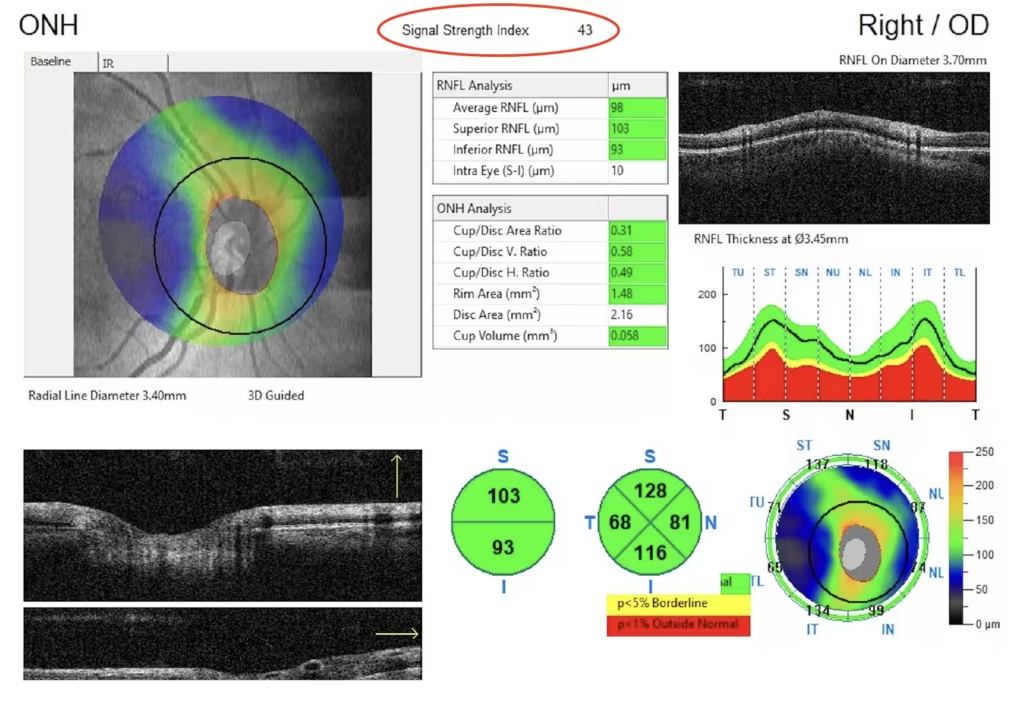
- Signal strength index (SSI) reductions of 15–25%.
- Signal-to-noise ratio (SNR) decreases of 20–30%.
- Higher scan failure rates, especially in severe DED.
- Increased retinal layer segmentation errors.
These changes are not just technical inconveniences—they can directly influence clinical interpretation.
OCT Parameters Most Affected by Dry Eye
Not all OCT measurements are impacted equally. Certain retinal analyses appear particularly vulnerable to tear film instability.
Retinal Nerve Fiber Layer (RNFL)
RNFL measurements are highly sensitive to image clarity. Tear film artifacts can artificially alter thickness values, potentially creating false signs of glaucoma progression or masking true disease changes.
Ganglion Cell Complex (GCC)
GCC analysis depends heavily on accurate retinal layer segmentation. In dry eye patients, segmentation failures are more common, sometimes resulting in unreliable or uninterpretable reports.
Macular Thickness Maps
Macular imaging may appear blurred or poorly defined when tear film quality is compromised. In some cases, this can mimic retinal edema, atrophy, or subtle structural abnormalities.
Why This Matters in Daily Practice
The clinical implications are significant. Imagine a glaucoma patient whose OCT shows apparent RNFL thinning during follow-up. Is it true progression, or simply poor image quality caused by tear film instability?
Without recognizing dry eye as a confounding factor, clinicians may:
- Escalate treatment unnecessarily.
- Order additional testing that may not be needed.
- Misinterpret progression trends.
- Miss early disease changes because imaging quality remains inconsistent.
For patients with chronic ocular surface disease, poor OCT quality can become a persistent barrier to accurate monitoring.
Practical Ways to Improve OCT Quality in Dry Eye Patients
Fortunately, several simple adjustments can improve imaging reliability in patients with DED.
Optimize the Ocular Surface Before Imaging
Use Preservative-Free Artificial Tears
Instilling preservative-free lubricating drops several minutes before scanning can help stabilize the tear film and improve optical clarity. However, overly viscous drops should be avoided immediately before imaging since they may introduce additional artifacts.
Encourage Proper Blinking
Patients often suppress blinking during OCT scans, which worsens tear breakup. Asking patients to blink fully several times before acquisition—and briefly rest their eyes closed for several seconds—can help redistribute the tear film more evenly.
Address Meibomian Gland Dysfunction
For patients with evaporative dry eye, warm compresses or lid hygiene before imaging may improve meibum quality and tear film stability.
Adjust OCT Acquisition Settings
Use Faster Scan Protocols
Shorter acquisition times reduce the chance of tear breakup occurring during the scan. Fast-scan settings can be especially helpful in symptomatic dry eye patients.
Be Careful With Excessive Averaging
While averaging multiple B-scans can reduce noise, longer acquisition times may worsen tear film instability and motion artifacts. Finding the right balance is important.
Utilize Low Signal Algorithms When Available
Some modern OCT platforms include algorithms designed to improve interpretation in lower-quality scans. These tools can be useful when ideal imaging conditions are difficult to achieve.
Knowing When to Repeat the Scan
Not every imperfect scan requires repetition, but clinicians should know when poor image quality compromises interpretation.
Consider Re-scanning If:
- Signal strength falls below manufacturer recommendations.
- Retinal segmentation fails completely.
- Significant dropout or streak artifacts are visible.
- Findings do not match the clinical examination.
Accept the Scan If:
- Artifacts are minor and major retinal structures remain visible.
- Signal strength is borderline but consistent across scans.
- Small segmentation errors can be manually corrected confidently.
Document Ocular Surface Findings
One simple but valuable habit is documenting tear film status in the OCT interpretation.
For example:
“OCT quality acceptable, though mild tear film instability noted. RNFL measurements should be interpreted cautiously given ocular surface findings.”
This provides important clinical context for future comparisons and may help explain variability between visits.
Integrating Dry Eye Management Into Imaging Workflows
As dry eye prevalence continues to rise, especially among older patients, more practices are incorporating ocular surface assessment into their imaging protocols.
Some practical workflow changes include:
- Screening for dry eye symptoms before OCT appointments.
- Allowing additional imaging time for patients with known DED.
- Training technicians to recognize tear film-related artifacts.
- Referring patients for dedicated dry eye treatment when imaging quality repeatedly suffers.
Improving ocular surface health benefits more than patient comfort—it also improves the accuracy and reliability of retinal imaging.
The Takeaway for Clinicians
Dry eye disease is more than a source of irritation or fluctuating vision. It is a genuine imaging confounder that can reduce OCT reliability and complicate clinical decision-making.
By recognizing how tear film instability affects OCT performance, clinicians can take simple but effective steps to improve scan quality, reduce artifacts, and avoid misinterpretation. Sometimes, the key to obtaining a better OCT image is not adjusting the machine—it’s treating the ocular surface first.

