Endophthalmitis: What Is It, Why Is It a Medical Emergency, and What You Need to Know
One of the most serious eye infections in medicine — and why acting fast is the only thing that can save your vision.
There are eye conditions that are uncomfortable. There are eye conditions that are concerning. And then there is endophthalmitis — a rare but devastating infection that sits in a category all its own. It is classified as a medical emergency. Without rapid treatment, it can permanently destroy vision in a matter of hours. And yet most people have never heard of it until they or someone they care about is diagnosed.
With endophthalmitis trending in health searches in 2026 — driven by new research, rising rates of eye procedures, and fresh clinical data — it is time to break down exactly what this condition is, who is at risk, what the warning signs are, and what modern medicine can do about it.
What Is Endophthalmitis?
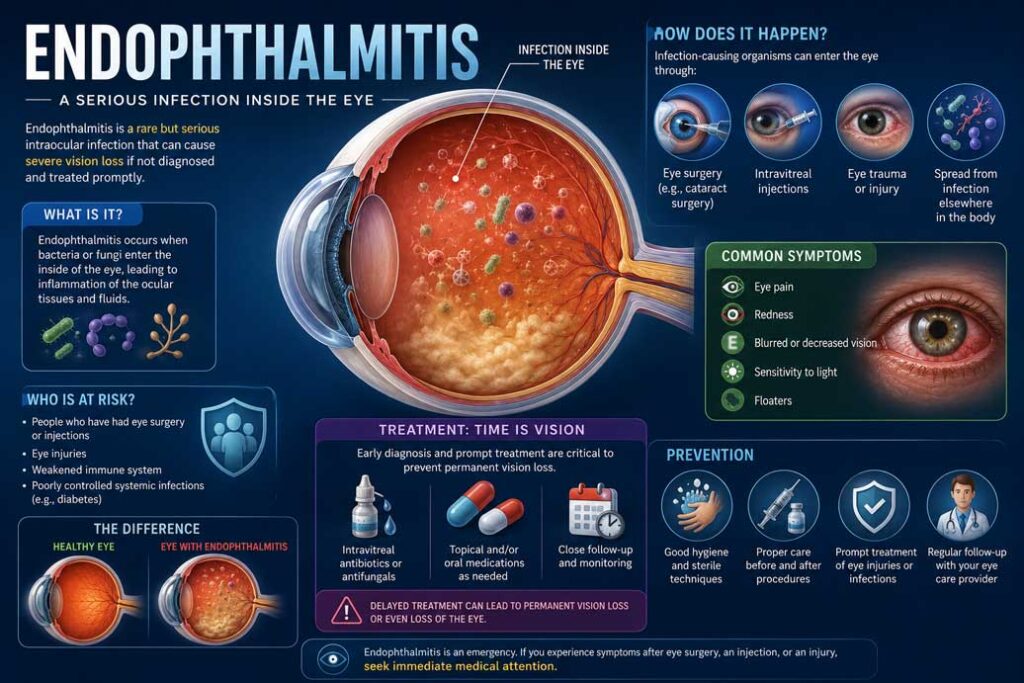
Endophthalmitis is a severe inflammation of the interior tissues and fluids of the eye — specifically the vitreous humor, the gel-like substance that fills the back of the eyeball, and the aqueous humor, the fluid in the front of the eye. In the vast majority of cases, this inflammation is caused by an infection — bacterial, fungal, or in rare cases, parasitic.
The name comes from the Greek words meaning “within the eye” and “inflammation.” That description is apt. Unlike an eye infection that affects the surface — such as conjunctivitis or a stye — endophthalmitis strikes deep inside the eyeball itself, where the body’s natural defenses have limited reach and where damage can escalate with frightening speed.
It is not a common condition. But its rarity offers little comfort to those who develop it, because the consequences of delayed treatment can be catastrophic and permanent.
The Two Main Types: Exogenous and Endogenous
Understanding endophthalmitis begins with understanding how the infection gets into the eye in the first place. There are two primary pathways.
Exogenous endophthalmitis is the more common type. Here, the infection enters the eye from the outside — through eye surgery, an injection into the eye, or a penetrating eye injury. Cataract surgery, which is one of the most frequently performed surgical procedures in the world, is one of the leading causes. Eye injections, which have become increasingly common for treating conditions like macular degeneration and diabetic eye disease, also carry a small but real risk. Traumatic eye injuries — particularly puncture wounds — are another significant cause.
Endogenous endophthalmitis is less common but often more difficult to diagnose. In this type, the infection does not enter from outside but rather travels to the eye through the bloodstream from an infection elsewhere in the body. Conditions such as bacterial sepsis, liver abscesses, urinary tract infections, pneumonia, dental procedures, intravenous drug use, and abscesses anywhere in the body can all serve as source infections. People with weakened immune systems — including those with diabetes, cancer, or those taking immunosuppressive medications — are at significantly higher risk of this form.
Between eight and twenty percent of endogenous endophthalmitis cases affect both eyes simultaneously, making early systemic diagnosis especially critical.
Warning Signs: Symptoms You Should Never Ignore
The symptoms of endophthalmitis can vary depending on the type and the organism responsible, but there are core warning signs that every person should know — especially anyone who has recently had eye surgery, an eye injection, or an eye injury.
The most common and alarming symptoms include sudden, severe eye pain, rapid and significant vision loss or blurring, intense redness of the white of the eye, swollen eyelids, and extreme sensitivity to light. Some patients also notice a yellowish or whitish discharge, floaters — dark semi-transparent shapes drifting across their field of vision — or a cloudiness or haziness in the eye.
One clinical sign doctors specifically look for is hypopyon — a visible accumulation of white inflammatory cells that settles at the bottom of the front chamber of the eye, creating a visible layer that resembles a small pool of cream. When present, it is a strong indicator of intraocular infection.
Bacterial endophthalmitis tends to present suddenly and dramatically, with symptoms escalating within hours to days. Fungal endophthalmitis, by contrast, tends to develop more gradually and can be deceptively subtle — some cases of fungal infection inside the eye are completely asymptomatic in their early stages, making them particularly dangerous because they may not be caught until significant damage has already occurred.
The critical rule is simple: if you have recently had eye surgery, an eye injection, or an eye injury of any kind — and you develop any of these symptoms — this is a medical emergency. Do not wait. Do not take a watch-and-see approach. Contact an ophthalmologist or go to an emergency room immediately.
How Is Endophthalmitis Diagnosed?
When a doctor suspects endophthalmitis, diagnosis must move quickly. The examination begins with a thorough assessment of the eye using a slit lamp, which allows the physician to see inside the eye in detail. Visual acuity testing, pupil response, and careful inspection of the anterior and posterior chambers are all part of the initial evaluation.
The definitive diagnostic step is a procedure called an aqueous or vitreous tap. Using a very fine needle, the doctor withdraws a small sample of fluid from either the front or the back of the eye. That fluid is sent to a laboratory where it is cultured to identify the specific organism causing the infection — bacterial, fungal, or otherwise. Identifying the pathogen is essential because the treatment varies significantly depending on the cause.
In some cases, an ultrasound of the eye is ordered to assess the extent of infection, particularly when visibility into the eye is limited by cloudiness or inflammation. Blood and urine cultures may also be ordered when endogenous spread is suspected.
Treatment: Why Speed Is Everything
Endophthalmitis is one of those medical conditions where the gap between prompt treatment and delayed treatment can be the difference between preserving vision and losing it permanently. Even a delay of a few hours can be catastrophic in acute bacterial cases.
The primary treatment for most cases of endophthalmitis is an intravitreal injection — an injection of antibiotic or antifungal medication directly into the vitreous cavity of the eye. This bypasses the blood-eye barrier that prevents systemic medications from reaching adequate concentrations inside the eye. For bacterial infections, broad-spectrum antibiotics are administered intravitreally while culture results are awaited, then adjusted based on the specific organism identified.
In more severe cases, or when the infection does not respond to injections alone, a surgical procedure called a vitrectomy may be required. During a vitrectomy, the infected vitreous gel is surgically removed from the inside of the eye, eliminating the bulk of the infectious material and allowing direct delivery of antibiotics into the cleared space. This procedure is more invasive but can be vision-saving in advanced cases.
For endogenous endophthalmitis — where the infection has spread from elsewhere in the body — treatment must also address the underlying systemic source. This typically involves intravenous antibiotics or antifungals alongside the eye-directed treatment.
Corticosteroids may be used in some cases to manage the inflammatory response, though their use remains a subject of ongoing clinical debate, particularly regarding timing and dosage.
New Research in 2026: What the Latest Data Shows
The medical community’s understanding of endophthalmitis continues to evolve, with significant new data emerging in 2026.
A major study presented at the Association for Research in Vision and Ophthalmology conference analyzed more than 430,000 intravitreal injections performed at a single center over five years. Researchers found that endophthalmitis rates remain very low across all intravitreal therapies — but importantly, the type of preparation matters. Patients who received injections from prefilled sterile syringes had lower infection rates compared to those whose injections were drawn from vials. The type of drug also appeared to matter, with corticosteroid injections carrying a higher infection risk than anti-VEGF treatments.
Separately, research on post-surgical endophthalmitis confirmed that cataract surgery patients had the lowest risk among all eye surgery types, while patients receiving secondary intraocular lens implants had the highest risk — findings that will help surgeons better counsel patients before procedures.
New prophylactic protocols are also showing promise. Studies examining the use of intracameral moxifloxacin — an antibiotic injected directly into the eye at the time of surgery — have demonstrated significant reductions in post-operative endophthalmitis rates, pointing toward improved prevention strategies for surgical patients.
Prevention: Reducing Your Risk
While endophthalmitis cannot always be prevented, there are meaningful steps that reduce risk significantly.
For surgical and injection patients, following all pre- and post-operative instructions precisely is essential. This includes using prescribed antibiotic eye drops as directed, avoiding rubbing or touching the eye, keeping the area clean, and reporting any new symptoms immediately — even minor ones.
For those at risk of trauma-related infection, wearing appropriate protective eyewear during contact sports, construction work, yard work, and any activity involving flying debris is critical. A moment of carelessness with eye protection can open the door to one of the most serious infections in medicine.
People with conditions that weaken immunity should be especially vigilant about any new eye symptoms and should ensure their treating physicians are aware of the connection between systemic infections and endogenous endophthalmitis.
The Bottom Line
Endophthalmitis is rare — but it is also unforgiving. It strikes fast, escalates quickly, and leaves little room for hesitation. The good news is that when caught early and treated aggressively, outcomes can be significantly improved. Vision can be preserved.
The message is straightforward: know the symptoms, understand your risk factors, and never minimize eye pain or sudden vision changes following an eye procedure or injury. When it comes to endophthalmitis, the clock starts the moment symptoms begin.
Your vision is worth acting on immediately.
Disclaimer: This article is for informational purposes only and does not constitute medical advice. If you are experiencing eye symptoms, seek care from a qualified ophthalmologist immediately.

