Trachoma: The World’s Leading Infectious Cause of Blindness and the Global Fight to End It
Millions of people are still at risk of going blind from a disease that is entirely preventable. Here is everything you need to know about trachoma in 2026.
It is one of the oldest recorded diseases in human history. Ancient Egyptian papyri described it. It has blinded soldiers, farmers, mothers, and children across centuries and continents. Yet in 2026, trachoma remains a stubborn threat — responsible for the blindness or visual impairment of nearly two million people around the world, almost all of them living in poverty.
At the same time, the global health community is making extraordinary progress. Countries that struggled with trachoma for over a century are now being declared free of the disease. The number of people at risk has fallen to historic lows. And a clear international roadmap exists to eliminate trachoma entirely by 2030. The story of trachoma in 2026 is both a sobering reminder of how far we still have to go — and an inspiring testament to what global cooperation can achieve.
What Is Trachoma?
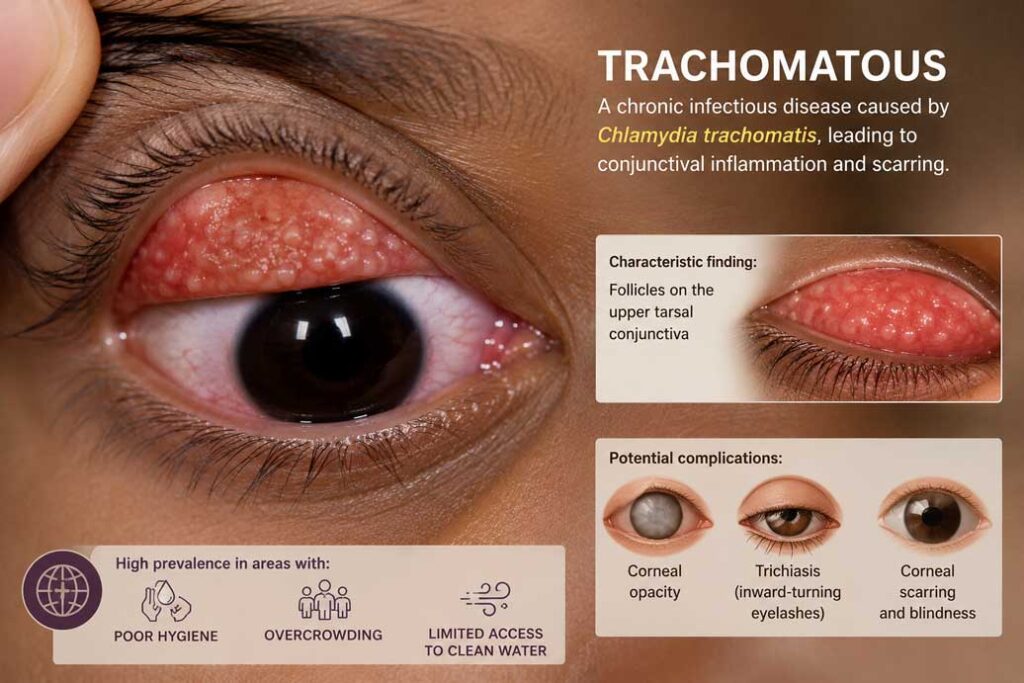
Trachoma is an infectious eye disease caused by a bacterium called Chlamydia trachomatis. It is the leading infectious cause of preventable blindness worldwide. Unlike sudden eye emergencies such as endophthalmitis, trachoma is a slow and relentless disease — one that causes blindness through repeated cycles of infection and scarring over years and decades.
The infection targets the conjunctiva, the thin membrane that lines the inside of the eyelids and covers the white of the eye. With each new infection, the inner surface of the eyelids becomes roughened and inflamed. Over time and with repeated reinfection, scar tissue builds up on the inner eyelid. Eventually this scarring causes the eyelid to turn inward — a condition called entropion — so that the eyelashes scrape directly against the surface of the cornea with every blink. This is as painful as it sounds, and the constant abrasion gradually clouds and destroys the cornea, leading to permanent, irreversible blindness.
What makes trachoma especially cruel is that the people it affects most severely are often not those who first caught the disease. Children in endemic communities are repeatedly infected from infancy, but the blinding consequences typically do not emerge until adulthood — often affecting women in their thirties, forties, and fifties who spent decades caring for young children and were unknowingly reinfected over and over again.
How Does Trachoma Spread?
Trachoma spreads through direct and indirect contact with the eye and nasal discharge of infected individuals. This can happen through hands, shared clothing, towels, bedding, and contaminated surfaces. Flies — particularly species attracted to the face — play a significant role in transmission in many endemic regions, carrying infectious secretions from one person to another.
Children between the ages of three and six are the primary reservoir of infection in trachoma-endemic communities. Their tendency to be in close physical contact with other children, combined with limited hygiene practices at young ages, makes them highly efficient transmitters of the bacteria. In some severely affected communities, the proportion of preschool children with active trachoma infection can be as high as ninety percent.
Women bear a disproportionate share of the disease’s burden. Because women are primarily responsible for child care in many trachoma-endemic settings, they are exposed to infection far more frequently than men, and as a result they develop the blinding complications of advanced trachoma at significantly higher rates.
The conditions that fuel trachoma are well understood: poverty, overcrowding, limited access to clean water, poor sanitation, and inadequate hygiene. Trachoma is, in a very direct sense, a disease of inequality.
The Five Stages of Trachoma
Trachoma progresses through five clinically recognized stages, each building on the damage of the last.
The first stage is trachomatous inflammation — follicular. This is the active infectious stage, common in young children. The inner eyelid develops small white or grey bumps called follicles — clusters of immune cells responding to the infection. At this stage, symptoms can resemble ordinary pink eye, including mild itching, watery discharge, and eye irritation. Symptoms typically begin within five to twelve days of exposure to the bacteria.
The second stage is trachomatous inflammation — intense. The infection becomes more severe, with pronounced redness, swelling, and thickening of the inner eyelid. Vision may begin to be affected as the cornea becomes involved. This stage indicates a heavier bacterial load and more significant risk of scarring.
The third stage is trachomatous scarring. Repeated infections have now left visible scar tissue on the inner surface of the eyelid. The white streaks or bands of scar tissue gradually distort the eyelid’s shape. This stage marks a turning point — while earlier stages are fully reversible with treatment, scarring begins a process that cannot be undone.
The fourth stage is trachomatous trichiasis — the most painful and dangerous stage before blindness. The accumulated scarring has pulled the eyelid inward, causing eyelashes to turn inward and rub against the cornea. Every blink is an act of self-inflicted injury. The pain can be debilitating, and untreated trichiasis leads almost inevitably to the final stage.
The fifth and final stage is corneal opacity. The relentless scratching of the inturned eyelashes has permanently clouded and damaged the cornea. Vision is severely reduced or lost entirely. This blindness is difficult to reverse and profoundly impacts quality of life, economic productivity, and independence.
Who Is Most at Risk?
Trachoma is a disease of specific geographies and circumstances. It is found predominantly in dry, arid regions near the equator, with the greatest burden concentrated in sub-Saharan Africa. It is also present in parts of Central and South America, the Middle East, Asia, and the Pacific.
Based on the most recent data, approximately 97 million people live in trachoma-endemic areas and remain at risk of trachoma blindness. Communities with limited access to clean water and sanitation, where hygiene practices are constrained by resource poverty, carry the heaviest burden.
People with weakened immune systems are particularly vulnerable to repeated and severe infection. Children are the most commonly infected, but women who care for children face the greatest long-term risk of developing the blinding complications of the disease. In communities where trachoma is endemic, it functions almost like a rite of passage — an invisible inheritance passed silently through generations.
Treatment: The SAFE Strategy
There is no vaccine for trachoma, but the disease is entirely preventable and treatable with the right interventions. The World Health Organization endorses a comprehensive four-pronged approach known as the SAFE strategy, which has become the backbone of global trachoma elimination efforts.
The S stands for Surgery. For those already in the trichiasis stage — where eyelashes are turning inward and scraping the cornea — corrective surgery is the only way to prevent blindness. The procedure involves repositioning or removing the inturned eyelashes to stop the ongoing corneal damage. In 2024 alone, more than 87,000 people received this sight-saving surgery.
The A stands for Antibiotics. The antibiotic azithromycin, generously donated by its manufacturer through the International Trachoma Initiative, is administered in mass drug administration campaigns to entire endemic communities. A single annual dose can clear active trachoma infections and dramatically reduce community-wide transmission. In 2024, more than 44 million people in endemic communities received antibiotic treatment.
The F stands for Facial Cleanliness. Regular face washing, particularly in children, is one of the most effective ways to break the cycle of transmission. Removing the eye and nasal discharge that harbors the bacteria — and keeping flies away from children’s faces — directly reduces the spread of infection within households and communities.
The E stands for Environmental Improvement. Access to clean water, proper sanitation facilities, and improved living conditions are fundamental to sustainable trachoma control. Without environmental improvements, the disease will simply return after antibiotic treatment ends.
2026 Update: Historic Progress Toward Global Elimination
The global fight against trachoma is producing results that would have seemed impossibly optimistic just a few decades ago, and 2026 has already brought major milestones.
In January 2026, the global population requiring interventions against trachoma fell below 100 million for the very first time — a watershed moment that reflects a 94 percent reduction in people at risk since 2002. This achievement is the result of decades of coordinated international effort, government commitment, and community-level action across some of the world’s most challenging environments.
In February 2026, the World Health Organization announced that Libya had eliminated trachoma as a public health problem — a historic victory for a country that had struggled with the disease for over a century and had faced significant obstacles including political instability and population displacement.
In April 2026, Algeria was validated by WHO as having also eliminated trachoma, joining a growing list of countries that have met the international elimination threshold. In May 2026, Tunisia became the 31st country globally to receive WHO validation for trachoma elimination, making it the first neglected tropical disease to be eliminated in that country.
As of mid-2026, a total of 31 countries have now been validated by WHO as having eliminated trachoma as a public health problem — a number that continues to grow as more nations complete their elimination programs.
The Road to 2030: What Still Needs to Happen
Despite this extraordinary progress, the work is far from finished. Trachoma remains a public health problem in around 30 countries. Significant funding gaps exist — an estimated 300 million US dollars is still needed to fill deficiencies in surgery, antibiotics, surveys, and research to achieve the 2030 global elimination target.
Many of the communities where trachoma persists are also the hardest to reach — affected by conflict, geographic isolation, limited health infrastructure, and extreme poverty. These are the last miles of the elimination journey, and they are often the most difficult.
The global health community’s target is clear: eliminate trachoma as a public health problem everywhere in the world by 2030. Achieving that goal will require sustained political commitment, continued antibiotic donations, expanded surgical capacity in remote areas, and long-term investment in clean water and sanitation.
What You Can Do
For most readers in Canada and other high-income countries, trachoma is not a personal health risk. But it is a cause that deserves attention and support. The organizations leading the charge against trachoma — including WHO, the International Trachoma Initiative, Sightsavers, and CBM — rely on public awareness, advocacy, and funding to sustain their programs in endemic regions.
Blindness from trachoma does not happen because of bad luck. It happens because of poverty, inequality, and the absence of resources that most of us take entirely for granted — clean water, soap, access to a doctor. That is a problem the world has both the tools and the knowledge to solve.
The progress of 2026 proves it is possible. What remains is the will to finish the job.
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Please consult a qualified healthcare professional for medical concerns.

